Yes, She Actually Said That
On the 25th of May 2014, the spokesperson for the Australian Vaccination Skeptics Network (AVSN, formerly the Australian Vaccination Network), Meryl Dorey presented a talk, Vaccinations – Do They Really Save Lives? at the Healthy Lifestyle (You Can Heal Yourself) Expo in Caloundra, Queensland.
If you’re familiar with the AVSN, you know they’re an anti-vaccine group that do not provide reliable information on vaccines, and in fact disseminate misleading, misrepresented and incorrect information about vaccination which engenders fear and alarm, according to the public statement the New South Wales Health Care Complaints Commission put out about them.
You may have heard of their spokesperson and public officer, Meryl Dorey, who has no qualifications in immunology, microbiology, medicine or vaccinology and who for over a decade has been the major voice behind most of the incorrect information put out by the group. This talk was no exception.
In reading the transcript there were three particularly egregious sections that showed a complete ignorance of immunology, and I must admit to enjoying falling down the rabbit hole of reading the broader history behind all three of them. So without further ado, Meryl Dorey’s own words, followed, of course, by referenced descriptions of the evidence around the claims.
Questioner: “Hi Meryl, thanks for coming along, Lee is my name. Uh I once worked with a bloke who had a severe allergy to peanuts, sesame oil and seeds. He had one mouthful one day, grabbed his throat and dived to his pocket for a pill. It was that quick, it fixed him but I only recently read something about the alleged cause of it but I don’t fully understand it, can you explain it in simple terms, something about the oil being used as a carrier to keep it effective for longer. Sorry on the um, um placebo, uh can you explain if I’m allowed to explain why, how many studies on vaccination effectiveness use uh adjuvants and you know, thiomersal as the placebo.”
Meryl Dorey: “Um, the peanuts, peanut oil we believe has been included in vaccines since the late 1960s. I am 56 years old, I was born in 1958. I never knew anyone with peanut allergies until I started having my own children. So for a long time, 30 years, I never knew about peanut allergies, now you don’t know anyone who doesn’t have them. And um, there’s an excellent book that I can recommend called “The Peanut Allergy Epidemic”, Heather Fraser I think is the name of the author, and she discusses it. Um they have evidence that peanut oil is used as a carrier in many vaccines and to this day it’s used in many vaccines. And because, probably too long to go into, but because vaccines are intended to alert your immune system to the fact that there is an invader in there, and if you attach a peanut oil, let’s say, or an oil, a lipid of some kind to uh, a virus or a bacteria and then you inject it into the body, the body can look at that and say, okay I see measles and I know that measles is an enemy – this is the theory and I don’t know if it’s true but this is the theory – I know that measles is an enemy and attached to that measles I’ve got this weird oil. Now I’ve got something in my body that looks just like that, uh, I have all of this myelin wrapping around my nerves, and other oils that my brain uses, so I’m going to attack this because it’s attached to measles and when I see this oil in something else, in something that I eat or in my body I’m going to attack that too. So I’m going to develop a peanut allergy, I’m going to develop anaphylaxis and I can die after peanuts.
The interesting thing is that in Asian countries, some Asian countries, peanuts are not common but um sesame seeds are, they use sesame seeds in their food, so in those countries we’ve been told that they use sesame oil in their vaccines and just the way that we have these peanut oil allergies, they have sesame allergies as well. So whether there’s proof of that, I don’t know, but it’s certainly interesting and it should be studied.”
The claim that peanut oil has been included in vaccines since the sixties is downright false, with peanut oil not in any vaccinations on the Australian or American schedules.
Only on anti-vaccines sites is this claim made. In lieu of any proof that vaccines currently contain peanut oil, the authors of those pages point to studies performed with experimental vaccines containing peanut oil based adjuvants, most citing papers detailing the development and eventual abandonment of ‘adjuvant 65-4’. As with any water-in-oil emulsion-based adjuvant, vaccine antigen was made up in water and an emulsifier used to suspend it in oil. However, unlike mineral oils which the body has difficulty clearing (and as such are not licensed for use in human adjuvants), the use of peanut oil in adjuvant 65-4 meant the oil was completely metabolisable. Contemporary studies showed a positive safety profile and duration of immunity in humans and animals for an experimental adjuvant 65-4-containing influenza vaccine, leading to a United Kingdom licence in 1973. However, the US requirement that the oil mannide monooleate be used instead led to reduced efficacy and saw the eventual abandonment of the entire adjuvant 65-4 vaccine project.
Similarly, sesame oil has been used experimentally in emulsion–based adjuvants.
The entirety of the evidence for the claim of peanut and sesame oils being in modern vaccines, as found on anti-vaccine sites, consists of links to early studies and reviews of peanut- and sesame-oil adjuvants, cited as somehow being proof they are included in current vaccines. In reality, the only emulsion-based adjuvants licensed for use in humans use the oil squalene.
A common trope to try and worm around this lack of evidence, used by many American-based anti-vax sites, is to say that because peanut oil is classified ‘generally regarded as safe’ (GRAS) by the United States Food and Drug Administration it does not need to be mentioned in the labelling of vaccines. However, a complete list of substances involved in vaccine production reveals that no peanut products are used at any stage of the process.
So Ms Dorey’s claim is presented not only without evidence but on investigation is found to be baseless, though oft-repeated in online anti-vaccine conspiracy websites.
But what about this part?
“And because, probably too long to go into, but because vaccines are intended to alert your immune system to the fact that there is an invader in there, and if you attach a peanut oil, let’s say, or an oil, a lipid of some kind to uh, a virus or a bacteria and then you inject it into the body, the body can look at that and say, okay I see measles and I know that measles is an enemy – this is the theory and I don’t know if it’s true but this is the theory – I know that measles is an enemy and attached to that measles I’ve got this weird oil. Now I’ve got something in my body that looks just like that, uh, I have all of this myelin wrapping around my nerves, and other oils that my brain uses, so I’m going to attack this because it’s attached to measles and when I see this oil in something else, in something that I eat or in my body I’m going to attack that too. So I’m going to develop a peanut allergy, I’m going to develop anaphylaxis and I can die after peanuts.”
Ms Dorey goes on to tell the questioner that the immune response generated against peanut oil in vaccines cross-reacts with myelin in the brain. While molecular mimicry – the phenomenon of an immune response against one molecule leading to an immune response against another similar molecule – is considered as a viable hypothesis for the development of demyelinating diseases, a literature search for the terms ‘peanut myelin’ fails to turn up any research demonstrating co-occurrence of peanut allergies with demyeinating disease, or any molecular evidence of immunological cross-reaction between antigens from either of these sources. Not only are peanut products not used in vaccine production, but there does not appear to be any evidence linking peanut allergies to demyelinating diseases as Ms Dorey claims.
The next excerpt contains a claim Ms Dorey has been making for a while now.
“And that sounds all well and good except we have known for over 70 years that the presence of antibodies do not mean that you are immune to the disease, in fact all it means is that you’ve been exposed because many people can have absolutely no antibodies to a disease and be immune to it and many other people can have very high levels of protective antibodies and not be protected. Um this is an obituary for Dr Merrill Chase, a man Merrill, and he is called the father of modern immunology and he discovered in the 1940s that it is not antibodies alone that protect us. The immune system is incredibly complex and uh a balanced, a wonderfully balanced system that, that, has been developed over millions of years in order to help protect us from the environment; from toxins, from diseases in the environment. And what Dr Chase found is that antibodies are only a small part of that process, they’re not the be all or the end all and that can explain why people who have very high levels of antibodies still get the disease. So the whole purpose of vaccination is to create these antibodies, to cause our bodies to create these antibodies, and yet that doesn’t mean that we’re going to be protected at all.”
This is a claim Ms Dorey has made before, specifically that vaccines are designed primarily to get B cells to produce antibodies against vaccine antigen, but because there exists another arm of the adaptive immune system (T cells, the cellular mediators behind Merrill Chase’s observations), and because antibodies are not an absolute marker of protection, vaccines therefore induce ineffectual protection.
First off, it must be pointed out, T cell responses induced by vaccines on the schedule have been researched and characterised.
However, what is particularly humourous about this claim is that knowledge of T and B cell interactions has actually been incorporated into vaccine design since even before the AVSN was founded. The conjugate Haemophilus influenzae type B vaccine, licensed in the United States since 1987, includes a protein carrier specifically chosen for its ability to stimulate T cells, to take advantage of the improved immune response that occurs when cell-mediated immunity and B cells cooperate.
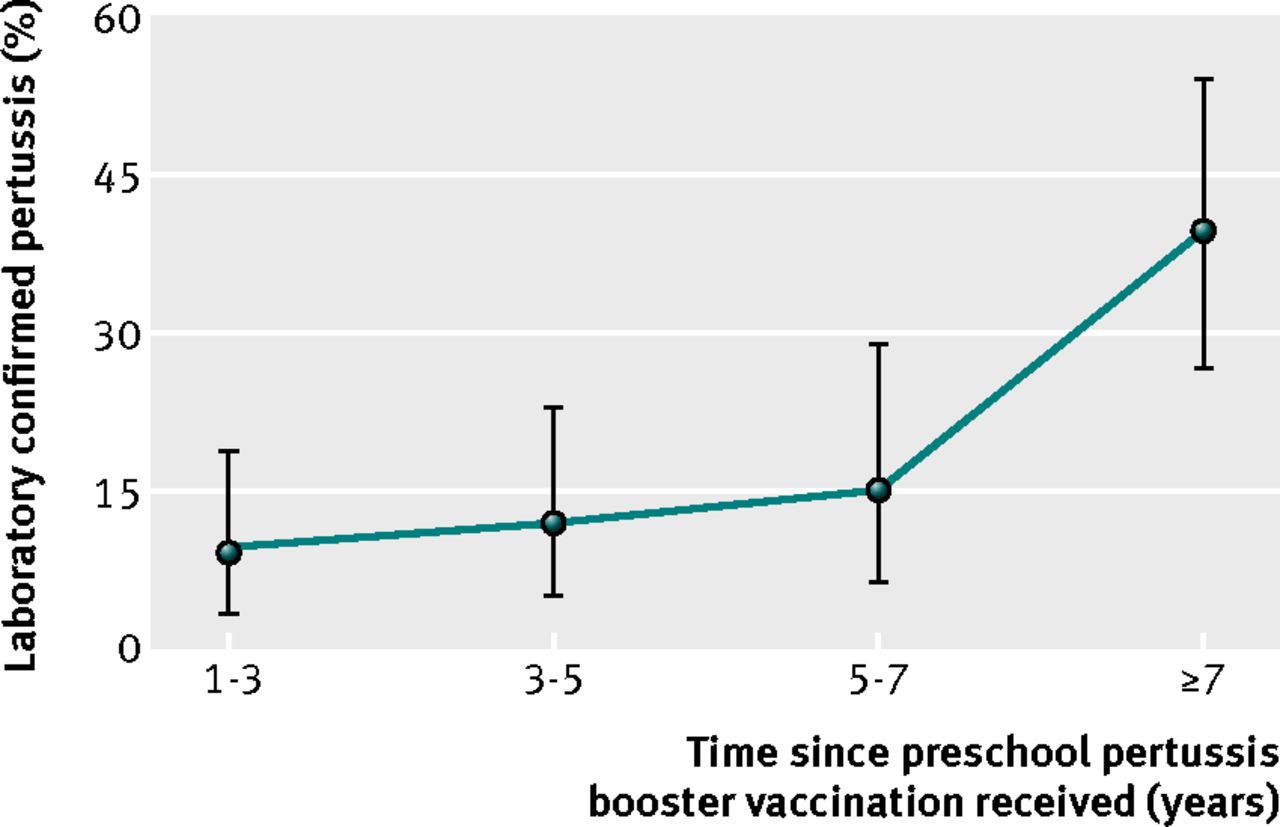
As for Ms Dorey’s claim that antibodies are no indication of whether you’re going to be protected at all, specific antibodies induced by vaccination are a quite effective indicator of the level of protection afforded to vaccine recipients. Decades of work show that by observing levels of antibody induced by vaccination and correlating it to disease outcome, it is possible to define a threshold of induced antibody above which an individual is at drastically reduced odds of developing disease on subsequent exposure. However, reduced risk of disease with high levels of antibody is not the same as no risk; the fact of the matter is that high levels of specific antibody correlate with a lower chance of catching disease, and better clinical outcome in those ‘breakthrough’ infections. However, the fact that small proportions of people may come down with disease despite being above an experimentally determined threshold does make Ms Dorey’s comment, “So the whole purpose of vaccination is to create these antibodies, to cause our bodies to create these antibodies, and yet that doesn’t mean that we’re going to be protected at all” technically true, if used entirely deceptively.
It’s worth pointing out that Ms Dorey’s dismissal of this work is not limited to rejecting the existence of an antibody-prognosis correlation simply because it is not absolute (the Nirvana logical fallacy), in fact she denies any immunological role for antibodies, outright describing them as “Peripheral to protection”, showing ignorance of decades of research that demonstrates protection mediated by direct transfer of antibodies, transfer of antibodies through breastfeeding and more recent highly specific mAb therapies.
Although one may suspect innocent oblivion on reading Ms Dorey’s diatribes that specific antibodies are nothing more than a marker of previous exposure, in the same post she cites as sources:
A review which describes in detail the protective levels of antibodies induced by vaccines, the evidence of antibodies as direct mediators of immunological protection and which, when it comes to the discussion of T cell responses, describes as “obvious” that “antibodies in sufficient quantity are the predominant protective correlate“.
A textbook chapter, which describes the importance of antibodies in mediating protection and paints a picture of T cell aspects of the response as primarily supporting antibody production.
A research paper in which mice whose B cells were unable to secrete antibody succumbed to an infection that wild-type mice survived (the authors go on to describe this antibody mediated protection as “critical” to surviving the infection) – an observation entirely incompatible with the antibodies being “peripheral to protection”.
Ms Dorey cites each of these as a source and yet continues to spread counter-factual information that they each refute, making it impossible to attribute this campaign of misinformation to mere ignorance. It seems Ms Dorey is either sufficiently scientifically illiterate to not realise the papers she cites for support are incompatible with her contentions, or she is deliberately deceiving the public about the efficacy of vaccines and basic cellular and molecular functions of the immune system.
In summary, Ms Dorey states in the quote:
1 – That mechanistically, vaccines cannot work – apparently unaware that the mechanism she states they omit has been harnessed for decades to improve vaccine efficacy; and
2 – That a major cellular mechanism by which protection through immunological memory is maintained is pure fiction, despite over a century of research demonstrating its reality.
Such egregious misinforming of the public simply does not constitute appropriate behaviour for a health care provider.
Perhaps the best part of the talk though:
“Questioner: Hello, my name is Melanie. Thank you for your talk, Meryl, it was really informative. I did some research recently about human foetus cells being used in vaccines and I got some information off you. My question is – and as you know a lot of aborted foetuses are sold to the pharmaceutical industry each year – if the mother is vaccinated of that foetus will any of that carry into the foetus negative or positive? [inaudible]
Meryl Dorey: I just want to make sure I have that question right. The question is uh, the foetuses of mothers, mothers who abort their foetus, hospitals sell those foetuses to vaccine and drug companies, right? Okay, and that’s true. Would vaccines that the mother have received actually be uh the antibodies from those vaccines be in the baby and I’m saying yes, they would because um, the aborted foetuses that were used to make the rubella vaccine and the other vaccines that use aborted foetal tissue, chicken pox and others. The reason they were selected is because their mother had had rubella or chickenpox and the antibodies were present in the foetus. So yeah, they would be I think, as far as I know.”
Meryl Dorey tells this questioner that a black-market trade of foetuses aborted from mothers infected with vaccine-preventable diseases exists, to supply the raw materials for making more vaccines against those diseases.
This is entirely false.
“…mothers who abort their foetus, hospitals sell those foetuses to vaccine and drug companies, right? Okay, and that’s true.”
Australian law prohibits trade in human body parts, with the National Health and Medical Research Council’s Ethics and the exchange and commercialisation of products derived from human tissue deferring to section 4.1.13 of the National Statement on Ethical Conduct in Human Research (2007) which states “There should be no trade in human fetal tissue.”
Further, foetuses are just not required for the ongoing production of vaccines.
In the 1960s two cell strains (WI-38 and MRC-5) were derived from legally medically-aborted foetuses. These cell strains simply need to be given the right conditions to survive and replicate; the progeny of those cells isolated in the ’60s are still used and dividing today in laboratories around the world. Because viruses need to infect living cells to replicate, the viral components of Hepatitis A, Rubella, Varicella, Adenovirus and Rabies virus vaccines are grown in those two cell strains. Vaccine production just does not need a periodic top-up of fresh fetuses as Ms Dorey says is provided by her fictional fetus-trade.
“The reason they were selected is because their mother had had rubella or chickenpox and the antibodies were present in the foetus.”
The cell strains were not chosen to grow these viruses because the mother was infected with them (firstly, there are two strains and five viral species cultured in them), they were chosen simply because they supported growth of those viruses. The mothers’ infection history and whatever antibodies they were passing on to their fetuses are entirely irrelevant to this. The presence of antibodies against the virus in question should be expected to be a hindrance to their culture, and could be expected to interfere with the action of the vaccine should they make it into the final product.
Ms Dorey’s talk shows ignorance of some basic concepts in immunology (such as what antibodies are, and a role of T-B cell interactions which has been incorporated into vaccine design longer than the AVSN has existed) and vaccine production (featuring a description of virus culture so fantastical it breaks Australian law). What is worse, Ms Dorey’s previous use of references that so neatly contradict so many of these claims makes it very difficult to believe these are simple naive mistakes.
No group that so radically and deliberately misinforms the public deserves the official status of healthcare provider that the Australian Vaccination Skeptics Network has.







{kind=link}